
A Glimpse into the Workplace of 2020. Are You Ready for Generation Y Managing Your Workplace?
By Unknown
I'm not. But with my soon to be 20 year old son coming home this week from a semester in Europe, it has me thinking. Here's an interesting blog post from greatplacetowork.com ...
First off, there is a shifting mix of employment/entrepreneurial/freelancing opportunities. Gone are the days when you were told to “do your time” as you began your career. This has shifted the leverage and attraction that big companies once had. In fact I would go as far as to question the talent shortage that we keep talking about. Perhaps there is no talent shortage, just a shortage of millennials who want to work in unprogressive organizations. But I digress…
The second shift in the workplace will be the centre of power. By 2020 Generation Y will outnumber the Boomers and many will be in decision-making roles. Generation Y will be poised to create the workplace they have always wanted.
Peer2Peer Value
Peer2Peer collaboration will be driven by the introduction of more empowering technologies & a preference for collaboration. More and more organizations will adapt a Google mentality – encouraging collisions and cross-pollinations between people for the sake of innovation! This will mean managers will focus away from managing individuals and towards getting more peer2peer value. Collaboration across the organization and with customers and suppliers will become the norm not the exception. This will mean that innovation and new ideas will come from everyone, regardless of your job box or title.
My Work, My Way
We will stop talking about work-life balance and flextime and move towards work-life integration. Generation Y managers will allow people to personalize the way they work to get things done (as long as the customer experience isn’t compromised). This philosophy is driven by Gen Y strong preference to have this control and autonomy of the way they work too. They don’t buy into “facetime”, seniority and other antiquated work concepts. If you can work anywhere, anytime then why should workplaces count the minutes. Plus technology will make it easy to get work done productively anywhere. The idea of standard office hours will become passé. People will be measured on providing a great customer experience, demonstrating personal productivity, efficiency and agility - all leading indicators to getting good results. If you can take off a day without impacting your clients, who cares. The organization saves money and you get what you want. No vacation policies common in start-ups will become common in large organizations.
Technology workarounds
Generation Y will not put up with systems that slow them down. The smartphones, apps, social networks, the cloud will all be brought into the workplace. This generation will find ways to work around Legacy systems or get rid of them where possible. As managers they will bring in more agile tools that make it simple to be productive. On the HR side, the use of video interviewing (Kira Talent), real-time performance systems (Work.com), social networking platforms (Yammer), company-sponsored learning channels (You Tube) and virtual and collaborative team meetings (Google Hangout) will become commonplace.
Good, bad and the ugly
In 2020 we will no long be sitting down for our annual performance appraisals (as least not in most organizations). Instead we will be used to constant, transparent feedback and recognition from our internal and external customers. Feedback will go up and down and all around if we follow the example of HCL Technologies where you give everyone feedback even your boss.
I am personally looking forward to being managed by a younger generation. Enjoy a glimpse into the workplace of the future where autonomy, service and just doing it creates excellence.
Generation Y – A Glimpse into Workplace of 2020
by Daneal CharneyJust wait until you grow up
What will generation Y be like as managers? Some argue that when Generation Y becomes managers they will adapt the same behaviors and practices as the rest of us. “Wait till they grow up and have real responsibility!. That will teach ‘em”. While this line of thinking seems to make sense because GenerationY will be in the same life stage (married, kids, etc) as the managers before them, it doesn’t take into account the tremendous shifts in the world of work.First off, there is a shifting mix of employment/entrepreneurial/freelancing opportunities. Gone are the days when you were told to “do your time” as you began your career. This has shifted the leverage and attraction that big companies once had. In fact I would go as far as to question the talent shortage that we keep talking about. Perhaps there is no talent shortage, just a shortage of millennials who want to work in unprogressive organizations. But I digress…
The second shift in the workplace will be the centre of power. By 2020 Generation Y will outnumber the Boomers and many will be in decision-making roles. Generation Y will be poised to create the workplace they have always wanted.
Gen Y Deal Breakers
In Bill Jenson’s Ten Year Report, he states that 20% of organizations have already adopted Work 2.0 environments. By the time Generation Y become managers, this number will increase markedly. The strong preferences of generation Y towards practices like peer2peer collaboration, results-only work environments, empowering technologies and real-time feedback will push us quickly towards Work 2.0. Here is what a workplace run by Generation Y will look like.Peer2Peer Value
Peer2Peer collaboration will be driven by the introduction of more empowering technologies & a preference for collaboration. More and more organizations will adapt a Google mentality – encouraging collisions and cross-pollinations between people for the sake of innovation! This will mean managers will focus away from managing individuals and towards getting more peer2peer value. Collaboration across the organization and with customers and suppliers will become the norm not the exception. This will mean that innovation and new ideas will come from everyone, regardless of your job box or title.
My Work, My Way
We will stop talking about work-life balance and flextime and move towards work-life integration. Generation Y managers will allow people to personalize the way they work to get things done (as long as the customer experience isn’t compromised). This philosophy is driven by Gen Y strong preference to have this control and autonomy of the way they work too. They don’t buy into “facetime”, seniority and other antiquated work concepts. If you can work anywhere, anytime then why should workplaces count the minutes. Plus technology will make it easy to get work done productively anywhere. The idea of standard office hours will become passé. People will be measured on providing a great customer experience, demonstrating personal productivity, efficiency and agility - all leading indicators to getting good results. If you can take off a day without impacting your clients, who cares. The organization saves money and you get what you want. No vacation policies common in start-ups will become common in large organizations.
Technology workarounds
Generation Y will not put up with systems that slow them down. The smartphones, apps, social networks, the cloud will all be brought into the workplace. This generation will find ways to work around Legacy systems or get rid of them where possible. As managers they will bring in more agile tools that make it simple to be productive. On the HR side, the use of video interviewing (Kira Talent), real-time performance systems (Work.com), social networking platforms (Yammer), company-sponsored learning channels (You Tube) and virtual and collaborative team meetings (Google Hangout) will become commonplace.
Good, bad and the ugly
In 2020 we will no long be sitting down for our annual performance appraisals (as least not in most organizations). Instead we will be used to constant, transparent feedback and recognition from our internal and external customers. Feedback will go up and down and all around if we follow the example of HCL Technologies where you give everyone feedback even your boss.
I am personally looking forward to being managed by a younger generation. Enjoy a glimpse into the workplace of the future where autonomy, service and just doing it creates excellence.
Labels: 2020, Generation Y, Work 2.0, workplace



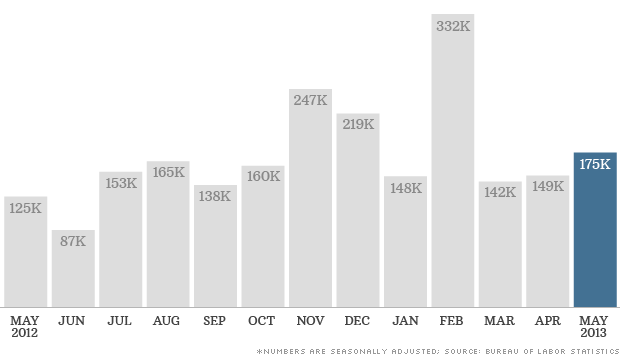 The U.S. economy added 175,000 jobs in May, in line with average job growth over the prior 12 months.
The U.S. economy added 175,000 jobs in May, in line with average job growth over the prior 12 months.